
Today all people 16 and older are eligible to get a COVID vaccination. Nationwide, about 40% of us have had at least one dose of vaccine, with >80% of those over 65 at least partially vaccinated, and more doses are coming fast and furious. It’s time to contemplate how this all comes to an end.
When the disease was starting out, it was recognized that left unchecked, every sick person would typically infect about three more people during the course of their illness. This disease infection rate, or reproductive factor, 
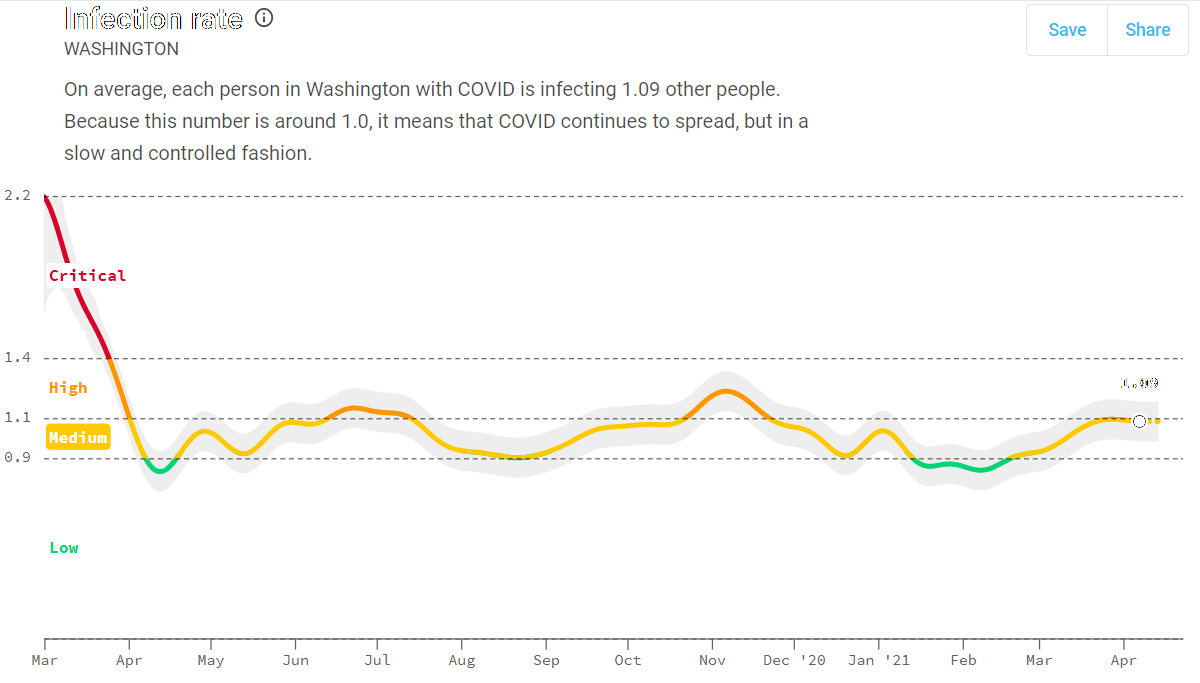
Other states with early heavy infections, New York, New Jersey and Florida, for example, had initial infection rates with 


Why is it so hard to sustain an infection rate less than one, as we see in the COVID Act Now graphs? There are a lot of moving pieces that generate the single infection rate number. A big one is the behavior changes we make because we are afraid of the disease. When we see refrigerator trucks filled with bodies outside of NYC hospitals, we take notice, stay in our homes and disinfect our mail and groceries before they enter the door. But our memories are short, we get convinced that this is just a case of the flu, and we stop being careful until the next surge of dead bodies. The progression of the disease has built-in delays and rate factors that allow significant amounts of infection to invade a locality before it is obviously a problem. Many cases of the disease are known to be asymptomatic yet still infectious. Disease from asymptomatic vectors is almost impossible to predict or control. As immunity to the coronavirus gradually increases in the population, the virus will find refuge in pockets of humanity with low immunity and groups with poor hygienic behavior. Person-to-person social networks which support the infection can generate islands of viral reserves. With more than 5.5 million employer businesses in the US, there will be a wide range of workplace attitudes toward the seriousness of the virus and the safety and efficacy of vaccination. Faith, political, and activist organizations may have large fractions of their members with opposition to vaccination or virus mitigation efforts such as mask wearing. Such social networks, where the disease can spread, will keep the virus circulating even as the general level of immunity and safe practices increases over time. This evening’s news mentioned Amish resistance to getting vaccinated, and that surplus vaccines are available in eastern Oregon where a new heated outbreak is in progress, yet less than 50% of the population has chosen to become vaccinated. We are only now beginning to run into vaccine reluctance as a determining factor for the continued pandemic.
COVID variants are another factor that makes containing the pandemic more of a challenge. There are now circulating several variants that appear to be more transmissible than the original virus. The figure below from the CDC shows how some of the variants have rapidly become much more common since the beginning of the year.
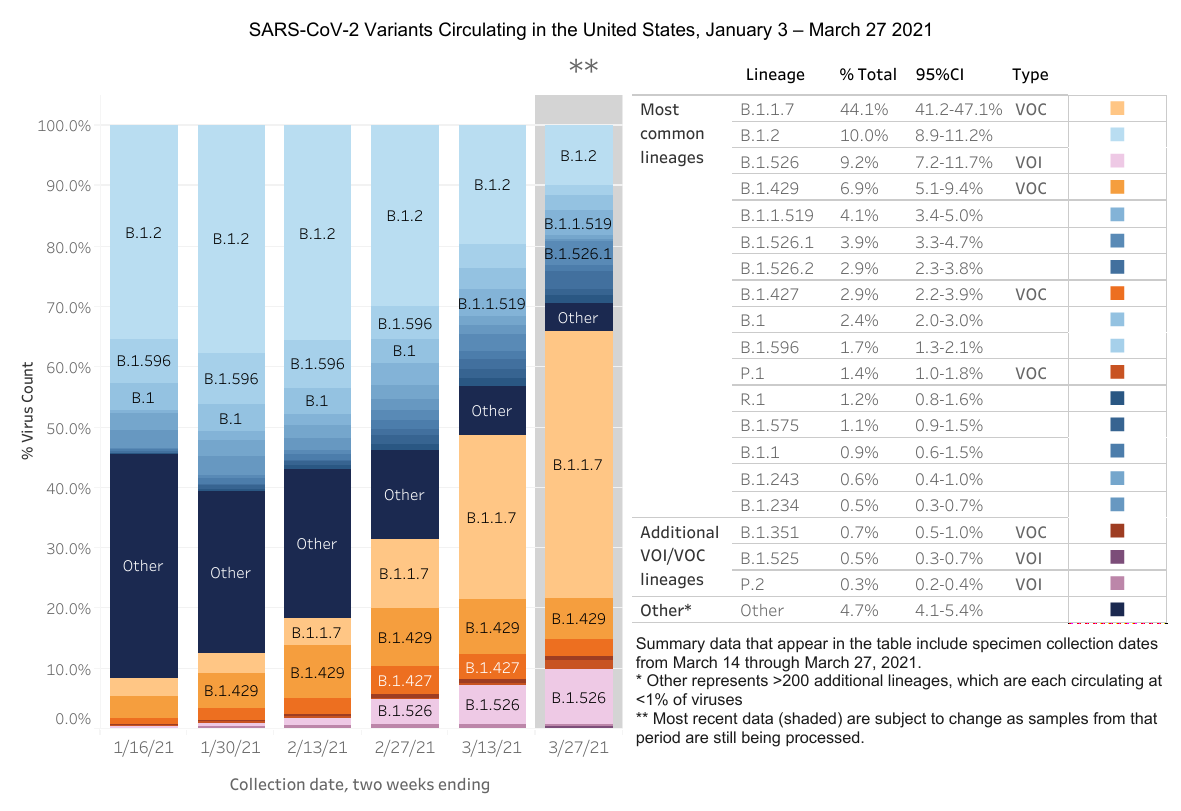
The “U.K. Variant”, B.1.1.7, is now the most prevalent strain in the United States. It is estimated to be 43% to 90% more infectious than the predecessor lineages.[2] More transmissible variants push 


Unfortunately, achieving control of more infectious agents require even more draconian preventative measures. That approach seems politically untenable at the moment, so the result will be a race between vaccine immunity and the immunity following a storm of infection. Fortunately, many of those most vulnerable to the worst ravages of the disease have already been vaccinated. Those questioning if they want to get the vaccine, perhaps with hopes that the disease will go away once many others have been vaccinated, should recalibrate their thinking, now that the new variants are controlling the ultimate progression of the pandemic. Eventually, 80% to 90% of us will have immunity to COVID-19, either through the vaccine or because we were sick. The risks associated with getting your immunity with a shot in the arm are much less dire than getting immunity because you have virus in your lungs and other body organs. In fact, 10% to 15% of those infected can develop “long COVID” symptoms, which can linger for weeks, even in younger patients with initially mild cases. This is not the choice way to gain immunity to further COVID infections.
Personal Risk Assessment
With many unvaccinated people in our midst, the virus still infecting large numbers of people, and vaccines that are not perfect, what are the risks for various types of activities for vaccinated individuals? First, let’s look at the big picture with what we know about the efficacy of the vaccines. The Pfizer and Moderna vaccines reported efficacy of 95% and 94% respectively against symptomatic COVID infection starting two weeks after the second shot. The Johnson & Johnson (J&J) vaccine reports about 66% efficacy against detectable infection and 85% at preventing serious illness. The J&J vaccine was tested when several mutant variants were widely circulating, so the numbers are not directly comparable. For my analysis, I will assume that the vaccines have about 90% efficacy. That means that of the general population that is getting sick with COVID, at least some will be “breakthrough” cases of vaccinated individuals. With 90% efficacy, you are 10 times more likely to get sick if you are not vaccinated than if you are vaccinated. However, the absolute probability that an individual will become infected also depends upon the probability that the individual will encounter other infectious individuals.
A recent study of infections at skilled nursing facilities (SNF) in the the Chicago area looked in detail at infections during and shortly after individuals in these facilities were vaccinated.[4] Of the approximately 14,765 residents and staff that were followed in the study, 22 were diagnosed with COVID infection after they were completely vaccinated. Significantly, most did not develop serious illness with 14 of the 22 not having any symptoms. Of the eight symptomatic cases, one died. During the study 447 individuals who were not yet vaccinated became infected with COVID and 14 died.
I made a rough estimate of the relative risks for infection before and after vaccination during the study period from Dec. 28, 2020 when first vaccinations were given, estimating that vaccinations were finished being administered by mid-February and everyone was past the 14 day waiting period by the end of February, until the end of the study period on March 31, 2021. In January and and early February, the Chicago area was seeing ~40 cases per 100,000 population (40/100k) per day. For the unvaccinated in the study, the rate was 97/100k during this same period, which is reasonable, since SNFs have always been virus hot spots. Once everyone had both shots, the rate of infection dropped to ~5.3/100k cases per day, dropping slightly more to 4.8/100k cases after waiting the additional 14 days. Meanwhile, the Chicago area generally improved from the situation earlier in the year to about 15/100k cases per day in late February and March. Taken together, this suggests that the SNF population went from being more than 2X more likely to be infected than the general population to being about 3X less likely to be infected than the general population after being vaccinated. The benefits are even better than suggested by these numbers, because even asymptomatic infections were picked up in the study participants.
Whether vaccinated or not, one’s risk of becoming infected is proportional to the prevalence of infectious persons we come in contact with. Hence, once vaccinated, it only makes sense to minimize risk of a breakthrough infection by mostly congregating with other vaccinated people. The 90% efficacy number suggests that your personal chance of being infected by any particular individual is 10 times less than it would be if you were not vaccinated. If the person you are in contact with is also vaccinated, then the risk of contacting the disease from that person drops to 100 times less than a contact between two unvaccinated individuals.
I tried to formalize the risk relationships, taking into account vaccination status, ongoing community infection rates, and gathering sizes with a simple spreadsheet calculator. A snapshot is shown below, and you can use the link below to download the calculator, so you can see what happens as the current daily case rate changes.
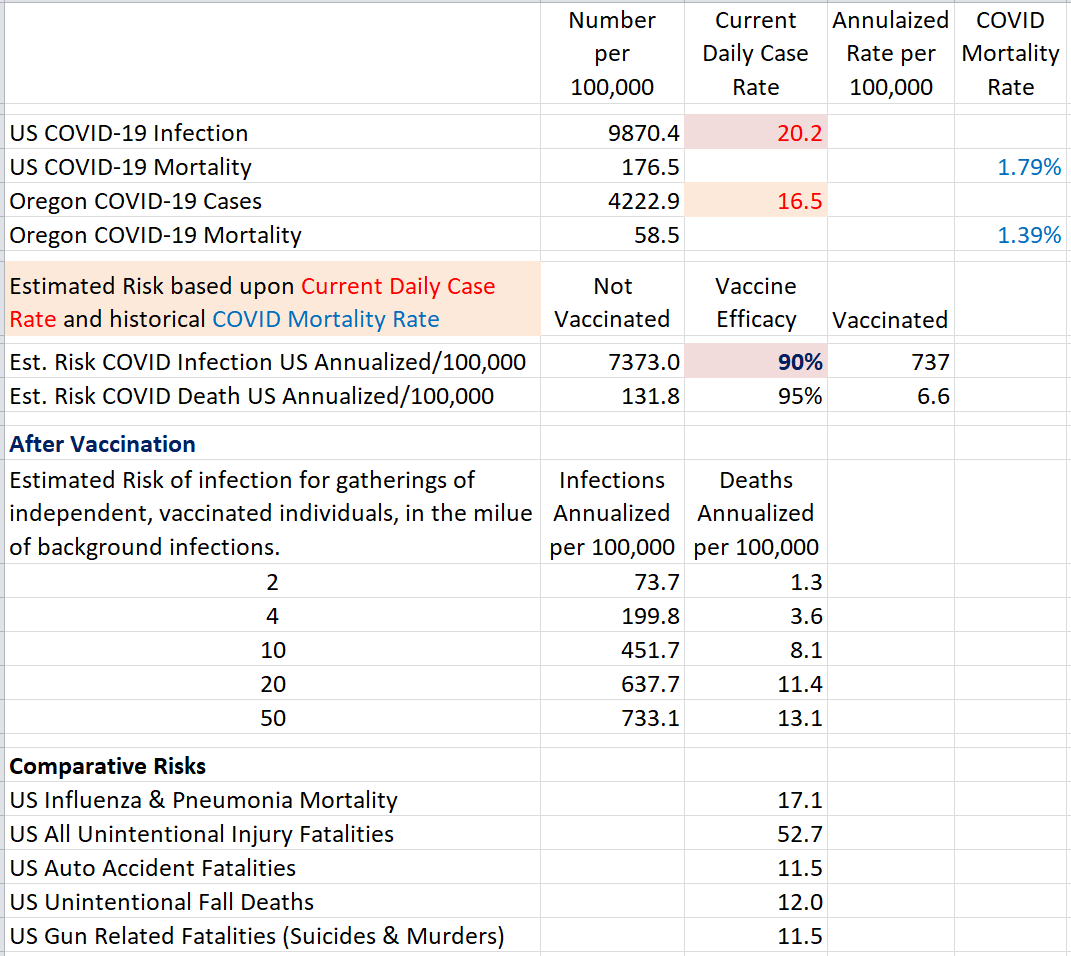
The background infection rate is driving the risk to everyone, including those vaccinated, because of the risk of breakthrough infections. The calculator uses the current US daily case rate, the top shaded box, to generate the various risk assessments. Estimated vaccine efficacy is also a free parameter for the calculator.
You can see that for gatherings of fewer than 10 vaccinated individuals, the risks will be very low. For large gatherings, there becomes the possibility of breakthrough cases, even if asymptomatic, that increase the risk as the number of people increase, until you are left with just your own vaccine efficacy to protect you. There is some evidence that the risk of infection from breakthrough cases is less than from non-vaccinated infectious people. Increasing the vaccine efficacy in the calculator could simulate such an effect.
Maybe a better way to look at personal risk is from a long-term perspective. Eventually the virus will come under control. It may remain endemic, mutating slightly to find chinks in our collective antibody armor, but no longer will the virus be “novel” and have a free reign on the general population. Children, who generally do not suffer badly from the disease, may become the reservoir of new individuals susceptible to the virus, keeping the virus alive long after the pandemic of 2020 is in the rearview mirror. This scenario suggests that pockets of virus will remain active for a long time, and that susceptible individuals will be at risk into the foreseeable future. With the new, more infectious variants, the herd immunity level may require that more than 80% be vaccinated, or have sustained a serious enough infection to generate long-lived antibodies. If vaccination efforts manage to get shots into 70% of the population, that still may leave a gap of more than 10% to achieve herd immunity, when the prevalence of the disease will finally naturally decline on its own. If you are one of the unvaccinated, and you are waiting for this desirable state of affairs, realize that it may require 1/3 or 1/2 or more of the unvaccinated to get sick with COVID to finally reach the herd immunity state. Hence, personal risk for the unvaccinated is very high, especially viewed on the long haul to the point where the disease is behind us. Time is not on the side of the unvaccinated.
References
- Achaiah NC, Subbarajasetty SB, Shetty RM. R0 and Re of COVID-19: Can We Predict When the Pandemic Outbreak will be Contained?. Indian J Crit Care Med. 2020;24(11):1125-1127. doi:10.5005/jp-journals-10071-23649
- Davies NG, Abbot S, Barnard RC, Jarvis CI, Kucharski AJ, Munday JD, Pearson CAB, Russell TW, Tully DC, Washburne AD, Wenseleers T, Gimma A, Waites W, Wong KLM, Van Zandvoort K, Silverman JD, et.al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England, Science 09 APR 2021.
- By Cmglee – Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=103529223
- Teran RA, Walblay KA, Shane EL, et al. Postvaccination SARS-CoV-2 Infections Among Skilled Nursing Facility Residents and Staff Members — Chicago, Illinois, December 2020–March 2021. MMWR Morb Mortal Wkly Rep. ePub: 21 April 2021. DOI: http://dx.doi.org/10.15585/mmwr.mm7017e1

Nice, Gary: Clear and useful. As usual. Any rough estimates protocol tenure? These masks are old already.
Once you are vaccinated, the additional protection from masks and distancing is minimal by comparison. All of those procedures reduced the collective transmission rates by about 2/3, whereas the vaccine reduces transmission by ~9/10. But right now it really comes down to supporting those not yet able to get the vaccine — mask wearing is a way of showing support and cognizance of the issue at hand. However, in your own home, with other vaccinated individuals — seems to me that we can go back to our old ways now.
Thanks Gary, great article. Seems so problematic that here in Lane County we are back in extreme risk category, but I heard that this is mostly due to student housing issues at UofO. So greatful to have gotten both doses done, and thankful to all the volunteers who make it happen so smoothly
Hi Jim,
Thanks for the comment. I guess it could be students locally, but the problem is statewide. We seem to have more than our share of the “California variants”. I noticed the spike in cases starting in the south coast counties a while ago. Meanwhile, because Oregon has done as good a job as it has at keeping cases low, we have a larger than average fraction of our people without any immunity acquired from the disease, so we are more prone to higher growth rate when these more infections variants show up. It’s a race we win if everyone gets vaccinated. Otherwise it could hang on with a slow rate of burn for quite a while.
GR